| No. | Description | Specification | Material |
|---|---|---|---|
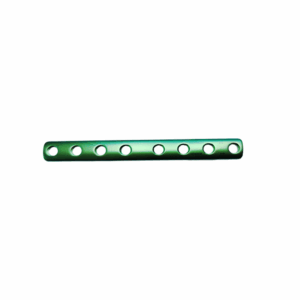
| 1 | FNS Locking plate | 1 hole | Titanium Alloy |
| 2 | FNS Locking plate | 2 holes | Titanium Alloy |
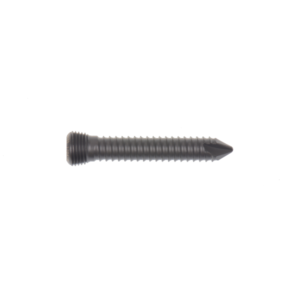
| 3 | Antirotation Screw | 6.5x80mm | Titanium Alloy |
| 4 | Antirotation Screw | 6.5x85mm | Titanium Alloy |
| 5 | Antirotation Screw | 6.5x90mm | Titanium Alloy |
| 6 | Antirotation Screw | 6.5x95mm | Titanium Alloy |
| 7 | Antirotation Screw | 6.5x100mm | Titanium Alloy |
| 8 | Antirotation Screw | 6.5x105mm | Titanium Alloy |
| 9 | Antirotation Screw | 6.5x110mm | Titanium Alloy |
| 10 | Antirotation Screw | 6.5x115mm | Titanium Alloy |
| 11 | Bolt | 10x80mm | Titanium Alloy |
| 12 | Bolt | 10x85mm | Titanium Alloy |
| 13 | Bolt | 10x90mm | Titanium Alloy |
| 14 | Bolt | 10x95mm | Titanium Alloy |
| 15 | Bolt | 10x100mm | Titanium Alloy |
| 16 | Bolt | 10x105mm | Titanium Alloy |
| 17 | Bolt | 10x110mm | Titanium Alloy |
| 18 | Bolt | 10x115mm | Titanium Alloy |
| 19 | Locking screw | 5.0x26mm | Titanium Alloy |
| 20 | Locking screw | 5.0x28mm | Titanium Alloy |
| 21 | Locking screw | 5.0x30mm | Titanium Alloy |
| 22 | Locking screw | 5.0x32mm | Titanium Alloy |
| 23 | Locking screw | 5.0x34mm | Titanium Alloy |
| 24 | Locking screw | 5.0x36mm | Titanium Alloy |
| 25 | Locking screw | 5.0x38mm | Titanium Alloy |
| 26 | Locking screw | 5.0x40mm | Titanium Alloy |
| 27 | Locking screw | 5.0x42mm | Titanium Alloy |
| 28 | Locking screw | 5.0x44mm | Titanium Alloy |
| 29 | Locking screw | 5.0x46mm | Titanium Alloy |
| 30 | Locking screw | 5.0x48mm | Titanium Alloy |
| 31 | Locking screw | 5.0x50mm | Titanium Alloy |
| 32 | Locking screw | 5.0x52mm | Titanium Alloy |
| 33 | Locking screw | 5.0x54mm | Titanium Alloy |
| 34 | Locking screw | 5.0x56mm | Titanium Alloy |
| 35 | Locking screw | 5.0x58mm | Titanium Alloy |
| 36 | Locking screw | 5.0x60mm | Titanium Alloy |
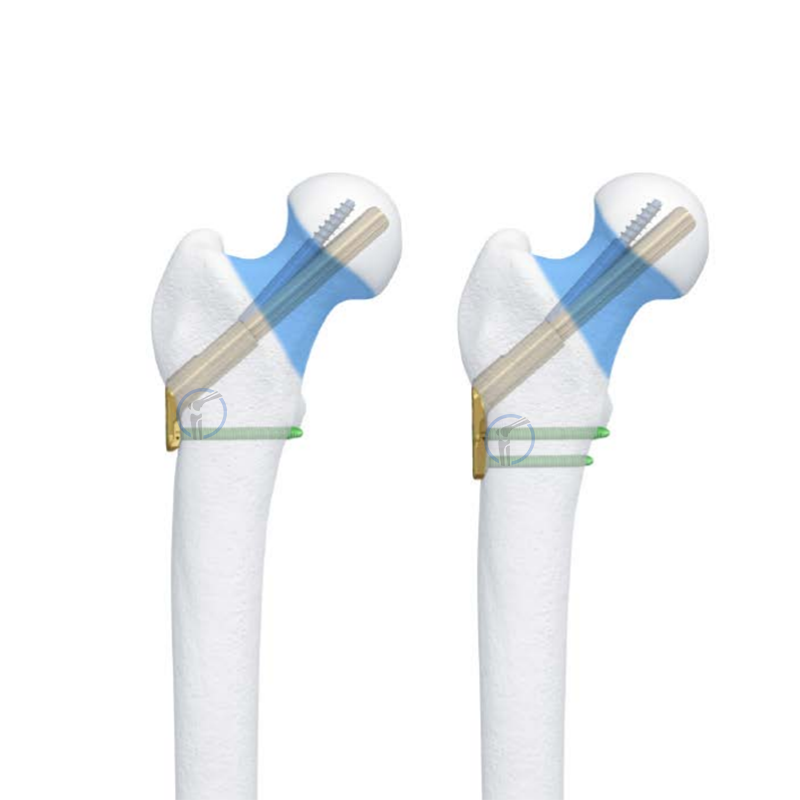
The Femoral Neck System (FNS) is a medical device designed to provide enhanced fixation for femoral neck fractures in adults and adolescents with fused growth plates.
Supine position on a fracture table or radiolucent operating table; traction applied for reduction. Ensure unimpeded fluoroscopic access (AP, Lateral, and true lateral views essential).
Obtain anatomical reduction under fluoroscopic guidance (critical for successful fixation). Closed reduction attempted first; open reduction via small anterior approach if necessary.
WhatsApp us